|
Questions & Discussions: (with potential answers) (Please answer the following questions commented from your RT attending physician.) |
| |
A1:
As described in the last attached page. (After your RT attending physician discussed with the radiologist by telephone, the radiologist confirmed preliminarily that no distant metastases were found based on the chest CT films, including lung to lung, liver, ribs & spine, and adrenal glands, and he said that some clinically significant lymph nodes over the contralateral mediastinum were found. Please further answer the following questions.)
A2:
cT4(direct mediastinum invasion)N3(contralateral mediastinum LNs)M0, stage IIIB, (2008/07, AJCC 2006)
A3:
No pathological stage can be defined, because no surgical resection was done.
A4:
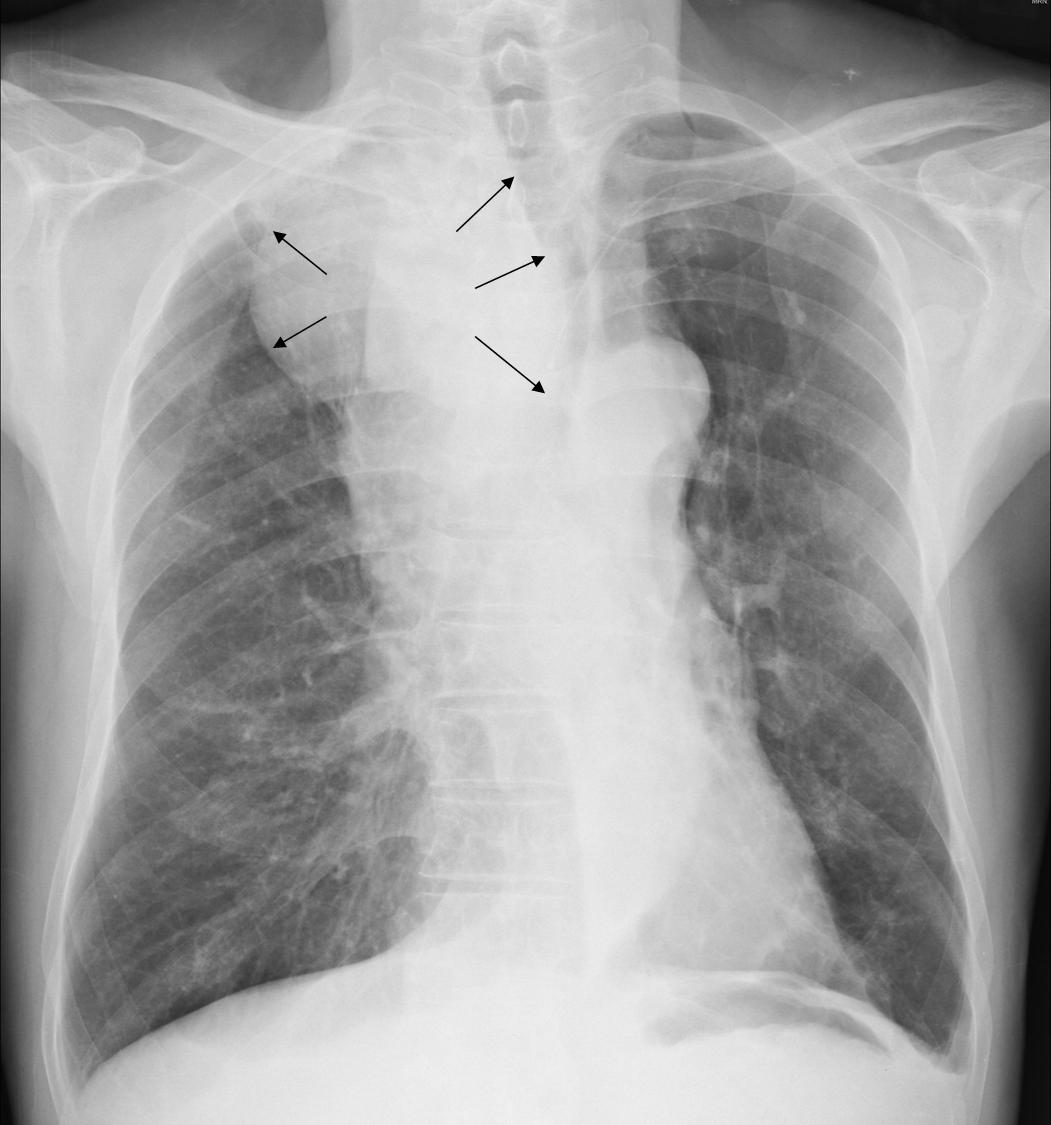
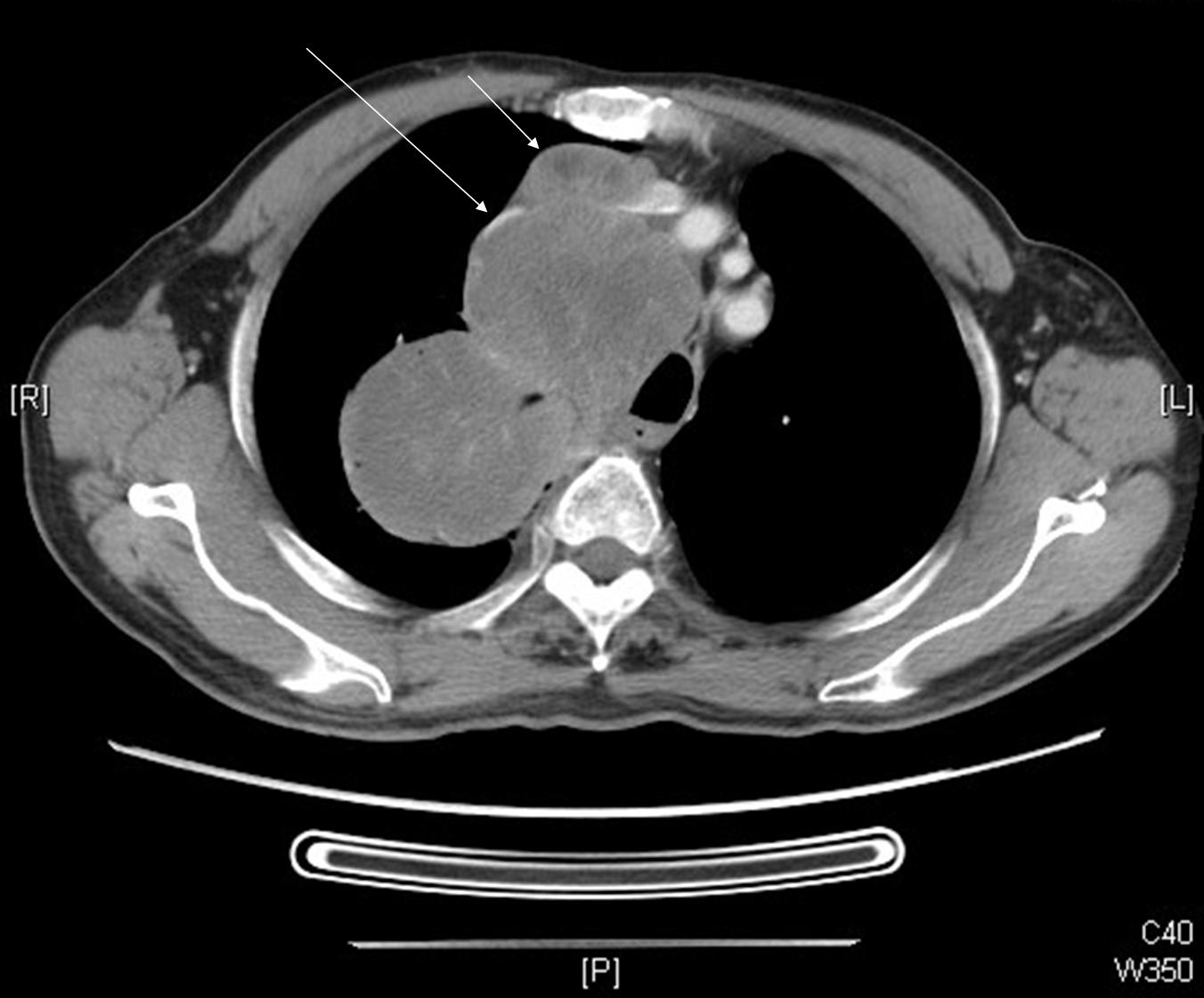
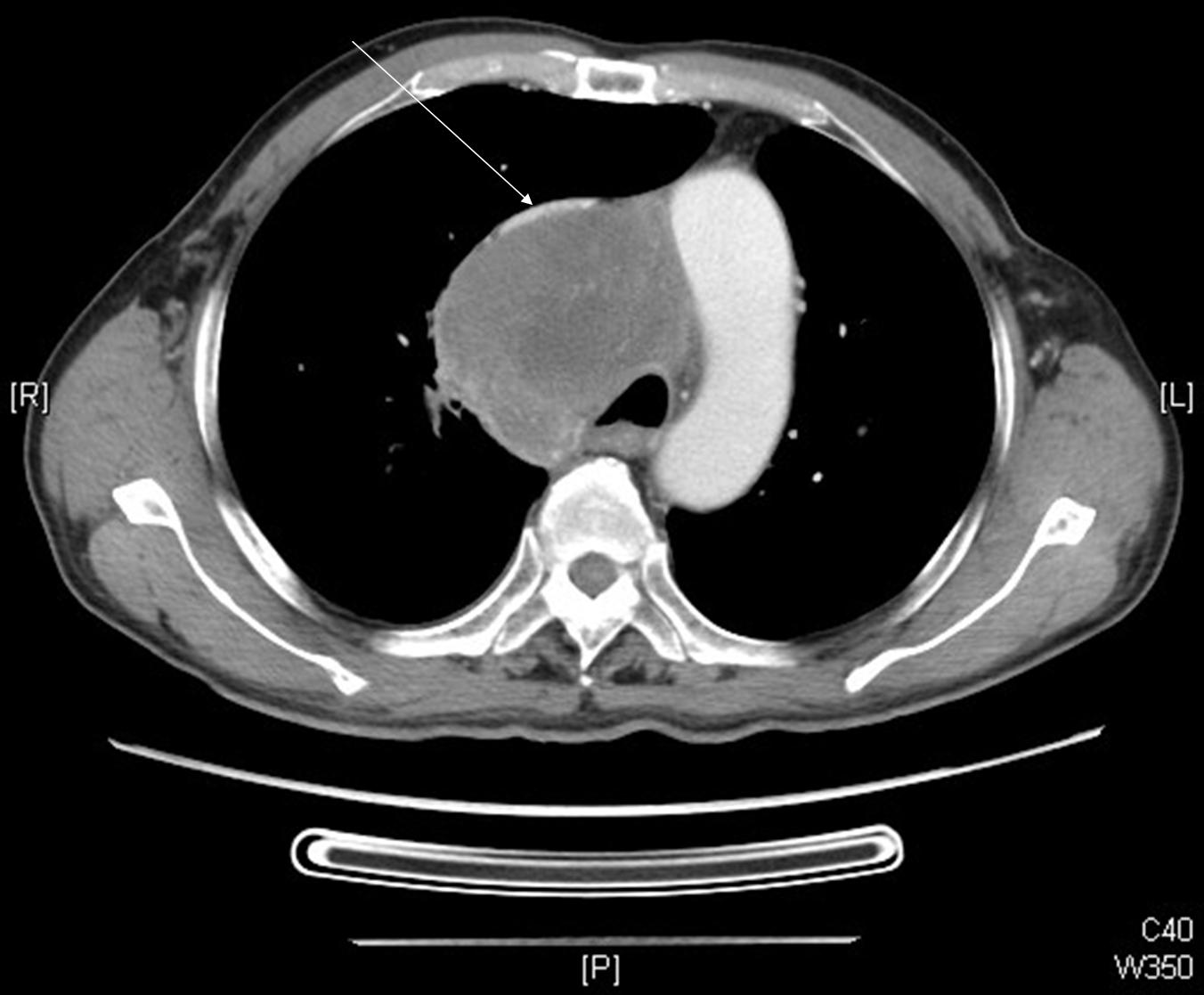
1. Oncology Diagnosis: Non-small cell carcinoma, poorly differentiated, of the lung, RUL, with mediastinum invasion, with mediastinum huge confluent LNs, with the trachea and the superior vena cava severe compression, cT4N3M0, stage IIIB, (2008/07, AJCC 2006); with LLL total collapse
2. Both chemotherapy and RT are indicated for this patient with the following indicators: Huge stage IIIB intra-thorax disease with compression of airway and superior vena cava
A5:
Planned CCRT according to NCCN cancer treatment guideline (2008)
A6:
RT Plan may be designed as the following one:
(1). Indication: Huge stage IIIB intra-thorax disease with compression of airway and superior vena cava
(2). Goal: potentially curative to palliative
(3). Target & Volume: gross tumor with adequate margin (0.5-1cm)
(4). Technique: 3DCRT
(5). Dose & Fractionation: 5040-5940 cGy in 28-33 fractions depending on patient’s performance status and V20 value of the lung in the RT treatment plan.
A7:
The patient is a case of pending SVC syndrome and is not a case of SVC syndrome. Because SVC syndrome is a clinical diagnosis based on clinical symptoms, it is not diagnosed based on incident image findings only. At visiting, this patient did not have typical symptoms of SVC syndrome, as follows: moderate to severe dyspnea; swelling/edema on the head and neck region, especially on the right side and the associated right upper limb; cutaneous/subcutaneous telangietaxia; cardiovascular symptoms due to SVC compression, such as palpitation, unstable blood pressure, and so on. But this patient still needs a prompt action intended to stop his clinical course change rapidly into a status of true SVC syndrome.
Further Readings & References: NCCN on-line cancer treatment guideline Radiation Oncologist Hon-Yi Lin 2008/08/30 |
|
|
Key Image(s): (with marked) |
| |
|